Skin Cancer Warning Signs:
Sunlight contains ultraviolet light that can have significant deleterious on human skin. Aside from skin aging these energetic light waves produce mutations in the DNA of skin cells which can accumulate to produce skin cancers. The incubation period can extend to decades. In areas close to the equator inhabited by individuals with poorly-pigmented skin, the incidence of cutaneous cancers is dramatically increasing. Since skin cancers are composed of masses of cells the most consistent warning sign is the development of a persistent bump or spot in an area of sun-damaged skin. Since these cancers require a blood supply they often exhibit small friable feeder vessels which are likely to bleed with minimal trauma and produce a superficial erosion.
Actinic Keratosis (Solar Keratosis)
Actinic keratoses are a rough scaly patch on your skin that develops from years of exposure to the sun. It is most commonly found on your face, lips, ears, back of hands, forearms, scalp or neck. An actinic keratosis begins slowly and usually causes no signs or symptoms other than a patch or small spot on your skin. A small percentage of actinic keratosis lesions can eventually become skin cancer. You can reduce your risk of actinic keratoses by minimizing your sun exposure and protecting your skin from ultraviolet (UV) rays. Limit your time in the sun. Especially avoid time in the sun between 10 a.m. and 2 p.m. Use sunscreen daily. Apply a broad-spectrum sunscreen. The American Academy of Dermatology recommends using a broad-spectrum, water-resistant sunscreen with an SPF of at least 30.
Actinic Keratosis

Actinic Cheilitis
Actinic Cheilitis (Farmer’s Lip)
Actinic cheilitis is simply actinic keratoses affecting the mucous membranes of the lips (vermillion border). This condition usually involves the lower lip simply because of the angle of incidence at which the overhead light waves hit the face. The forehead, cheeks, nose, and lower lip receive light waves perpendicularly and are not shaded by anatomical structures like the brows.
Cutaneous Horns
A cutaneous horn is a mass of dead skin cells. Essentially they have a lot in common with hair and nails since these are also composed of dead skin cells. The base which generates the horn can be an actinic keratosis, a squamous cell carcinoma, or a benign keratosis. The only way to differentiate between the three is by performing a surgical procedure called a biopsy and having it examined by a laboratory.

Cutaneous Hornes
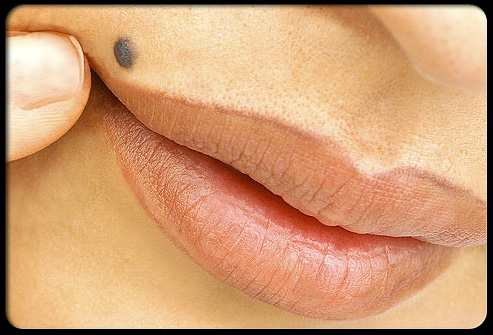
Dangerous Moles
When Is a Mole Dangerous?
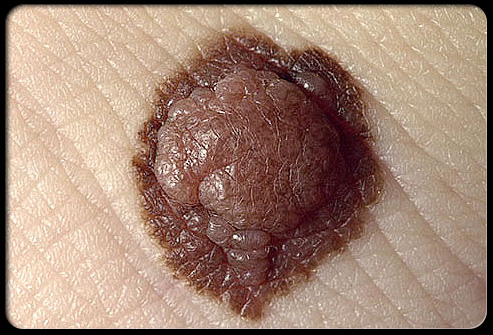
The word “mole” is probably derived from a German word meaning spot. When used in a cutaneous context it often refers to a spot on the skin. Since there are a variety of benign and malignant skin growths which fulfill this description, more precision is necessary. Moles that are melanocytic nevi (nevus singular) are local growths of melanocytes which can be present at birth or may develop after birth well into the third decade. They vary in color from black to flesh-colored. The number of moles present on a particular person is most closely related to skin color and the extent of exposure to sunlight during childhood. The average number of moles is about 35 per person in Northern European populations.
Atypical Moles
When a physician examines a particular nevus it can appear either ordinary or peculiar. The degree of peculiarity for better or worse has been called “atypicality.” This is a very imprecise descriptive term. There are families whose individual members have a great many very peculiar nevi and have a genetic predisposition to develop cutaneous melanomas. Most of these atypical nevi — when examined under the microscope — are not cancer; it seems to be the new lesions that develop in adulthood that are the ones that are most likely to be malignant melanomas. The term dysplastic refers to changes noted in moles that can only be appreciated on microscopic examination. This term should only be used when describing the microscopic appearance of a nevus or other tissue. Most atypical nevi exhibit some degree of dysplasia under the microscope.

Atypical Moles

Know Your ABCDEs
Know Your ABCDEs
In an attempt to systemize nevus description physicians use a variety of adjectives to describe visible alterations. To simplify things, benign lesions are almost always uniform in color, circular in shape, and exhibit bilateral symmetry about any axis drawn through its diameter. Malignant melanomas diverge from this appearance to a greater or lesser extent. To help one remember the criteria, they have been called the ABCDEs (mnemonic) of nevus description. Another valuable consideration is the so-called “ugly duckling” nevus which appears significantly different than all the other nevi on the patient.
‘A’ Is for Asymmetry of ABCDEs
Asymmetry refers to the degree of similarity when one compares the appearance of each of four quadrants produced by an imaginary cross through the middle of a melanocytic nevus.

‘B’ Is for Border of ABCDEs
Border refers to degree of circular regularity of the edge of a pigmented lesion. Perfectly circular lesions are rarely malignant.

‘C’ Is for Color of ABCDEs
Color: The degree of uniformity of color is a measure of atypicality. The more colors present the more likely the lesion is to be malignant.

‘D’ Is for Diameter of ABCDEs
Diameter: Although malignant pigmented lesions tend to be larger than a pencil eraser this is one of the less reliable criteria for distinguishing melanomas.
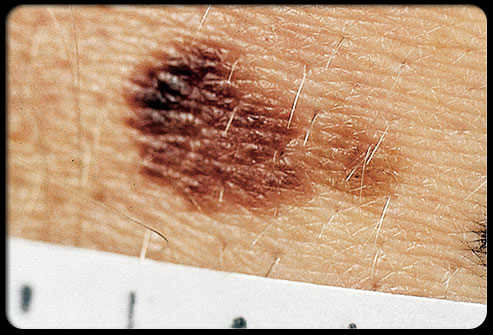
‘E’ Is for Evolving of ABCDEs
Evolving: Malignancies by their very nature tend to change over time — mostly by increasing in size — as opposed to benign lesions that are stable. Since cancers grow in an uncontrolled way they tend to produce asymmetrical lesions.
Screening Moles for Cancer
If a mole looks or acts at all peculiarly it is best to have it evaluated by an expert. This frequently is a dermatologist. Most dermatologists can tell if the pigmented lesion is composed of melanocytes or is something quite different with no possibility of being a melanoma. Many dermatologists now use a hand-held magnifying device which produces polarized light to evaluate colored melanocytic tumors. The use of this instrument improves the doctor’s ability to identify suspicious lesions.

Screening Moles for Cancer
Evaluations of Moles
Evaluations of Moles
The decision on which melanocytic lesions need to be examined depends on the concern the doctor has that it may be cancerous. Since the procedure necessary to take off the suspicious bump is simple, requiring only local anesthesia and rarely is associated with complications, the threshold for this procedure is appropriately low. If the lesion is melanocytic in origin and it appears at all peculiar, exhibiting any of the features addressed in the ABCDE criteria and/or the patient complains that the bump bleeds or is irritated or itchy, that is often enough to trigger a biopsy.
A Briefing on Skin Cancer
Malignant melanoma is the most deadly form of skin cancer because it tends to spread at a very early stage to other parts of the body. The likelihood that it has spread is most directly related to the thickness of the melanoma as measured from its surface to its depth by a pathologist. This information is communicated to the doctor that submitted the nevus and subsequent treatment depends on this information.

A Briefing on Skin Cancer

Melanoma
Melanoma
Although it is possible for a previously benign mole to become malignant most of the time a melanoma begins as a single malignant cell in previously normal skin and then continues to grow in an uncontrolled manner.
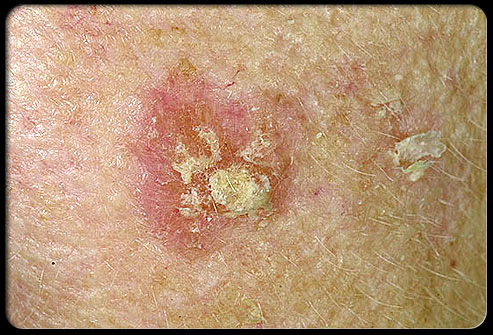
Squamous Cell Carcinoma
Squamous cell carcinomas begin as malignancies of living epidermal cells which grow and invade into the deeper layers of the skin. They usually begin as an actinic keratosis and progress over many years. Although most actinic keratoses do not eventuate into squamous cell cancers, if one has a great many of them and they continue to receive sufficient ultraviolet irradiation producing sufficient mutational events, it is extremely likely that a squamous cell carcinoma will develop. They appear as thick, keratotic bumps on sun-exposed skin which continue to enlarge. They do not commonly spread to distant sites, but larger lesions can do this.

Squamous Cell Carcinoma

Bowen Disease
Bowen Disease
Bowen's Disease typically presents as a gradually enlarging, well-demarcated red colored plaque with an irregular border and surface crusting or scaling. Bowen's disease may occur at any age in adults, but is rare before the age of 30, most patients are over 60. The cells in Bowen's disease are often highly atypical under the microscope, and may in fact look more unusual than the cells of some invasive squamous cell carcinomas. Treatments include cyrotherapy (freezing, topical chemotherapy and excision. Because the cells of Bowen's disease have not invaded the dermis, it has a much better prognosis than invasive squamous cell carcinoma.
Basal Cell Carcinoma
Basal cell carcinomas arise from the layer of skin cells present along the lowest layer of the epidermis and are the most common form of skin cancer. Fortunately they rarely spread to distant sites unless they are permitted to attain gigantic proportions. They are locally aggressive so they ought to be treated before they get so large that removal becomes technically difficult. The tumor has a shiny surface, is pearly white in color, and tends to bleed quite easily. It often ulcerates.

Basal Cell Carcinoma
Who Is At Risk for Skin Cancer and Why?
Sunlight is by far the most common cause of skin cancer. Most of the exposure occurs during leisure time or as a consequence of a desire to darken one’s basic skin color. The perceived benefits of exposure to sunlight seem to be confined mostly to the production of vitamin D in the skin, a belief that darker skin is more aesthetically appealing, and the warmth produced as the light as hits the skin. Vitamin D requirements can be easily satisfied with dietary supplementation. Light-skinned individuals with blonde or red hair who live in regions near the equator are most likely to develop skin cancer.
Reduce Your Skin Cancer Risk
It is important to avoid exposure to sunlight as much as is reasonably possible. Any time there has been a darkening of the skin after sun exposure it is a sign that some damage has been sustained. Since the incubation period for skin cancers and photoaging is quite long (5 to 15 years), it may be difficult to convince sun worshipers of the foolishness of this behavior. The use of clothing, searching for shade, and the application of effective, broad-spectrum sunscreens are all useful behaviors in limiting photodamage. Sunscreens that block all the wavelengths of ultraviolet light with an SPF (Sun Protection Factor) of 50 and that are reasonably durable are currently available.